In blood transfusion, component separation, and cell therapy, acid citrate dextrose (ACD) stands out for its reversible action, safety, and low cell toxicity. Two main ACD formulas—ACD-A and ACD-B—share the same basic chemistry but differ in key ways. This guide walks you through their anticoagulant principles, ingredients, physical properties, clinical and lab uses, handling tips, selection strategies, and common questions to help you choose and use them with confidence.
Table of Contents
Introduction
What is ACD-A?
ACD-A (Anticoagulant Citrate Dextrose Solution A) is widely recognized and used in clinical PRP systems. It’s composed of:
- Citric acid (22.0 g/L)
- Sodium citrate (81.0 g/L)
- Dextrose (glucose) (24.5 g/L)
This formula acts by chelating calcium, thereby stopping the coagulation cascade. It also helps maintain platelet integrity and function for a longer time after blood is drawn.

Benefits of ACD-A in PRP
- Preserves platelet viability over extended periods
- Maintains pH balance better during centrifugation
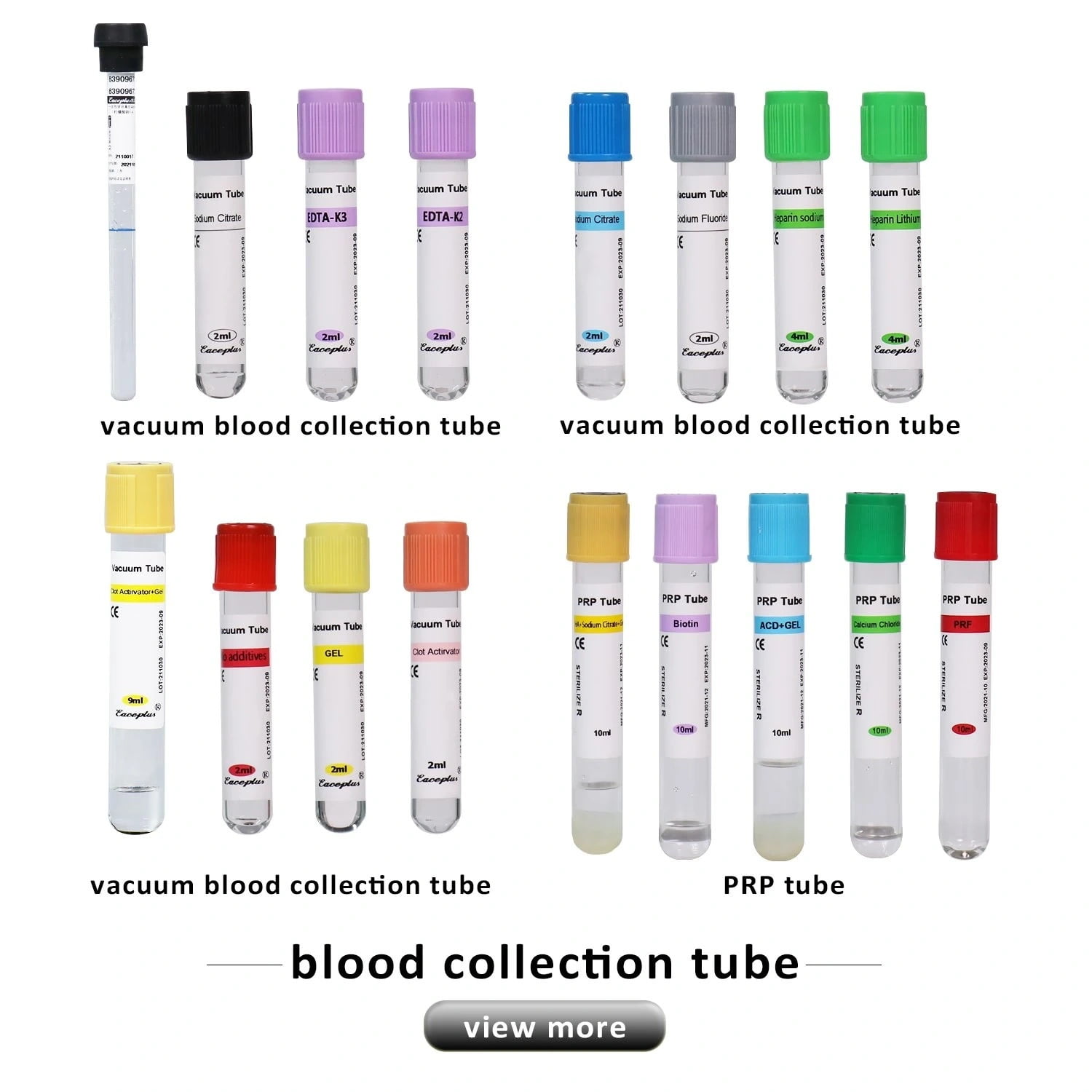
- Optimal for high-quality, clinical-grade PRP Tube
- Preferred in orthopedic, facial rejuvenation, and hair restoration procedures
For those sourcing PRP tubes pre-filled with ACD-A, check out the ACD Medical PRP Tube from SINY Medical. It’s lab-tested and designed specifically for professional-grade applications.
What is ACD-B?
ACD-B (Anticoagulant Citrate Dextrose Solution B) is a lesser-used version and has a slightly different concentration:
- Citric acid (13.2 g/L)
- Sodium citrate (44.0 g/L)
- Dextrose (14.7 g/L)
As you can tell, ACD-B contains lower concentrations of all components. This can affect the platelet activity and preservation quality.

Features of ACD-B in PRP
- Less acidic than ACD-A
- Shorter platelet preservation window
- May cause faster degradation of platelets
- Often used in basic or non-clinical PRP setups
How ACD-A and ACD-B Stop Clotting
- Calcium binding: Citrate ions form soluble complexes with free calcium in plasma, halting the calcium-dependent steps of blood clotting almost immediately.
- Reversible action: Once treated blood returns to the body, and the liver and muscles metabolize citrate through the citric acid cycle, freeing calcium again. You can reverse anticoagulation quickly by giving supplemental calcium if needed.
- Cell protection: Unlike heparin, ACD doesn’t interfere with platelet activity or trigger the complement system. This gentler action protects cell membranes and functions during separation or storage.
Key Ingredients and Physical Traits
- Citrate concentration: ACD-A contains about 2.2 g/L of sodium citrate, giving it rapid, strong anticoagulant power. ACD-B has around 1.32 g/L, which balances anticoagulation with a milder impact on cells.
- Glucose level: ACD-A provides roughly 2.0 g/L of glucose to fuel cells in the short term. ACD-B raises glucose to about 2.2 g/L, supporting high-activity cells like stem or immune cells over longer periods.
- pH and buffering: ACD-A sits around pH 4.5–5.0, acting fast but posing more stress on cell membranes. ACD-B maintains pH 5.5–6.0, easing stress and better preserving cellular integrity.
- Anticoagulant speed vs. cell care: ACD-A works faster, making it ideal for urgent large-volume draws and quick plasma separation. ACD-B acts steadily and offers stronger cell protection—perfect for long extracorporeal runs and storage.
Where to Use Each Formula
- Emergency large-volume blood draws & plasma exchange: Use ACD-A when you must anticoagulate large blood volumes quickly. Watch calcium levels closely and add calcium back as needed.
- ECMO and long extracorporeal circulation: ACD-B’s steady action and gentler pH help prevent complications like low calcium and cell damage during extended runs.
- Stem cell and immune cell harvest, storage, and infusion: ACD-B reduces cell death and preserves cell function, boosting success rates for transplants and therapies like CAR-T.
- Platelet preparation and research: Citrate has minimal effect on platelet aggregation, so you can study platelet function or sort cells under near-natural conditions using ACD-B.
Handling Tips and Precautions
- Mixing ratio: Keep blood to ACD at about 9:1 to 12:1. This ratio prevents clotting without diluting blood or upsetting electrolytes.
- Temperature and mixing: Bring anticoagulant and blood to the same temperature (room temperature or 37 °C). Gently invert tubes 5–10 times instead of shaking to avoid cell damage.
- Maintain sterility: Use opened ACD within two hours. Wear sterile gloves and masks, and avoid repeated punctures or open containers to reduce infection risk.
- Calcium replacement before reinfusion: For long runs or large transfusions, give 5% calcium gluconate or 10% calcium chloride about 10–15 minutes before reinfusion. Aim for ionized calcium of 1.1–1.3 mmol/L.
- Monitor pH and electrolytes: Check blood gases every 1–2 hours during extended circulation. Track pH, bicarbonate, sodium, potassium, and chloride, and adjust with bicarbonate or electrolyte solutions as needed.
How to Choose and Use
- Fast, high-volume needs: Pick ACD-A for emergency draws and quick plasma work.
- Long runs and cell care: Choose ACD-B for ECMO, extended circulation, and sensitive cell handling.
- Special patient groups: For children, the elderly, or people with heart or kidney issues, ACD-B’s milder acidity reduces risks.
- Research labs: Use ACD-B for platelet studies, flow sorting, and cell culture to minimize variability.
Final Thoughts
Choosing between ACD-A and ACD-B in PRP is more than a technical detail — it directly impacts treatment success, patient safety, and therapeutic outcomes.
To recap:
- ACD-A: Best for rapid processing, high-yield PRP, and aesthetic/clinical use.
- ACD-B: Better for gentle handling, long extracorporeal circuits, and sensitive cells.
When in doubt, go with trusted suppliers like SINY Medical, who offer tested, sterile, and GMP-compliant PRP tubes for every need. Their experts are also available to help guide your product selection — just reach out here.
Want a one-stop source for clinical PRP solutions? Browse their full product line on Made-in-China.
FAQ
Why use citrate instead of heparin?
Citrate halts clotting by binding calcium, spares platelets, and reverses quickly with calcium. Heparin works through antithrombin III, can cause platelet drops (HIT), and takes longer to reverse.
How do I check acid stress on cells?
Combine blood gas pH readings with cell viability tests (e.g., trypan blue staining) and flow analysis of cell markers to gauge cell health after storage or circulation.
What if the pH drops below 7.30?
If blood gas shows pH < 7.30, infuse sodium bicarbonate (1–2 mmol/kg) and adjust based on follow-up measurements and patient condition.